

Babies & Breakthroughs: The Updated IVF
Babies & Breakthroughs: The Updated IVF
The story of the first IVM-birth in Australia, and all things test-tube babies

A few days ago the first aussie baby was born that was conceived via a new infertility treatment called In-Vitro Maturation (IVM). IVM is a type of Assisted Reproductive Technology (ART). I’m probably not helping very much definition wise, but ARTs are fertility treatments used to help one achieve pregnancy. That can be for couples having difficulties doing so or single parents wanting to have a child. An ART is basically any sort of fertility treatment in which eggs or embryos are handled outside of a woman’s body. The most famous and common is In Vitro Fertilisation (IVF), with Louise Brown being the world’s first 'test-tube baby' born 45 years ago in England!
IVM has been nicknamed the low-cost IVF alternative which clearly also plays a big role to patients. It probably doesn’t sound that exciting to you currently but I’m hoping by the end of this essay you will get my excitement (outside of my personal bias to the topic for those of you who know me…)
So, let’s get started! 💃🏻
1. The art of ARTs
Background
ARTs were created to support with infertility, now that may be due to male, female, or combined causes (and sometimes unknown too). The top level idea is that you take an egg and sperm cells and place them in an in-vitro environment, meaning a petri-dish. There a zygote (a fertilised egg) should form which hopefully / ideally develops into an embryo that is then transferred back into the womb.
Fun (?) Fact: in-vitro means “in glass” and as the embryo forms in a “test tube” instead of in the fallopian tube, that’s where the term test-tube babies comes from, truly a non-medical one…
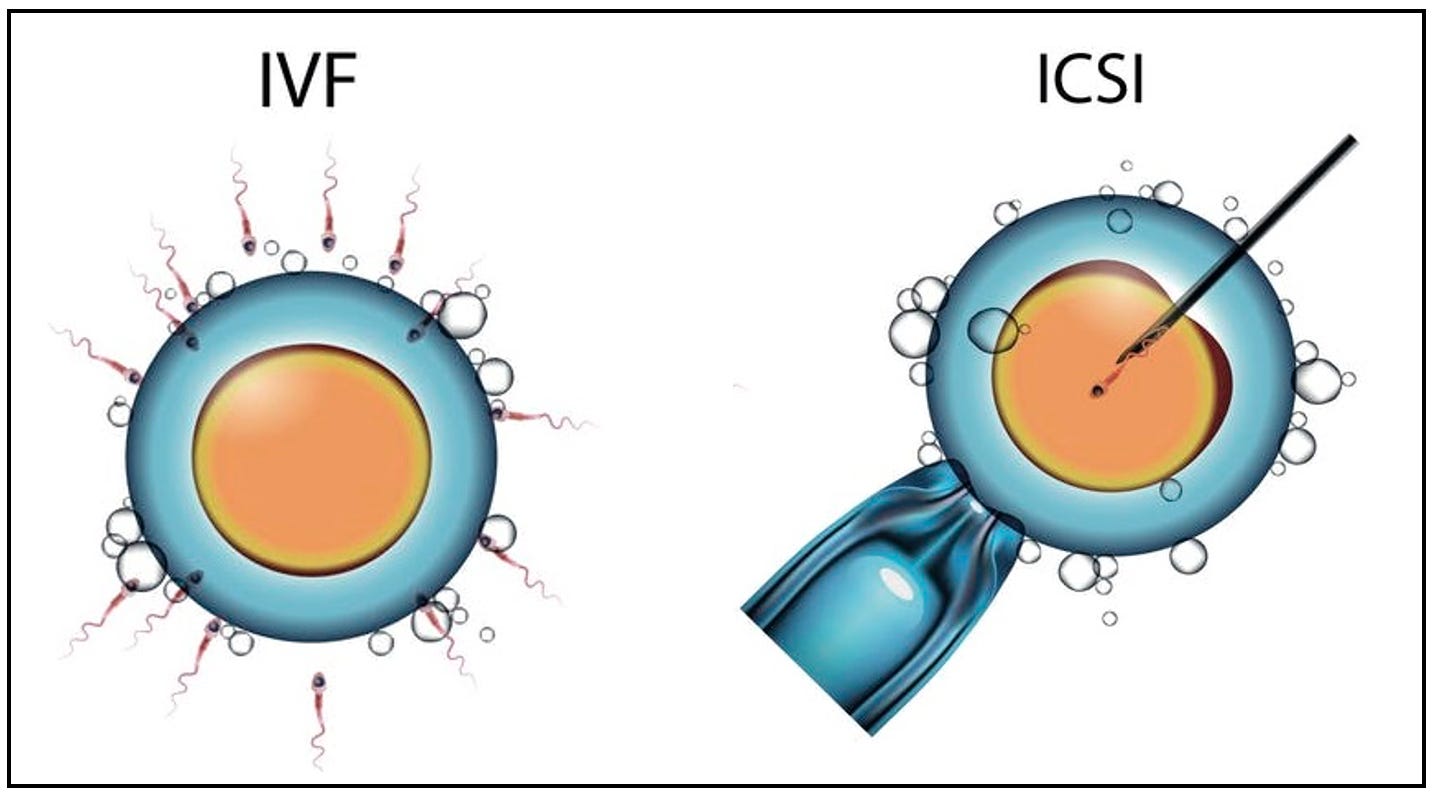
The main two ARTs are IVF and ICSI. ICSI stands for intracytoplasmic sperm injection and it’s not used as much since it’s beneficial in couples with male factor infertility, but also used in the case of sperm donors.
Now, the preceding steps for both treatments are identical up until the fertilisation point. The main difference is that in IVF sperm cells are added to the petri dish where the egg is and the best one fertilises the egg, while in ICSI the sperm is injected into the egg under the microscope with a tiny needle. Again, post fertilisation the steps are also identical. Another differentiator is that ICSI is much more expensive than IVF.
Egg Retrieval
I won’t cover the medical side and cause(s) of female factor infertility, but, a very important part of these treatments is around the egg retrieval and its quality. Typically a woman would either undergo a process to collect her own eggs so they can be fertilised or use donor eggs (those may be fresh or frozen and the donor would have undergone that process instead).
Side note - the reason as to why a couple may end up using donor eggs are many, these could be:
older women that didn’t manage to get any good eggs during the collection process
in the case of successful retrieval the eggs didn’t become embryos during the fertilisation process
multiple failed rounds of IVF and due to the patient’s age and probability of a successful pregnancy will be significantly higher using donor eggs
women that underwent medical treatments when younger which had an adverse affect on their fertility, for example chemo
women that experienced early menopause
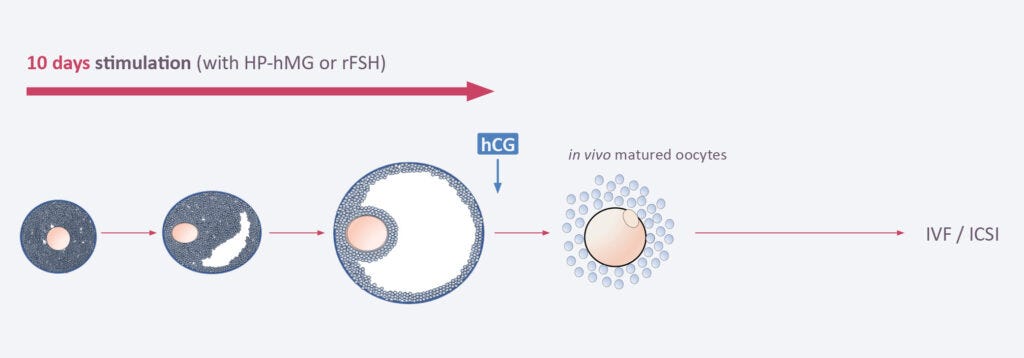
The reason that IVM is much more appealing to patients, cost aside, is the process of egg retrieval. With IVF stimulatory fertility drugs are used for around 2 weeks which help ovaries produce multiple eggs. With IVM the eggs are collected from the ovaries while they’re still immature without or with minimal stimulation. They’re then grown in a lab for 1-2 days and then undergo the fertilisation process. Under normal circumstances, one ovary releases a single egg per cycle, although very few women have both ovaries releasing an egg; this is also the reason for fraternal twins outside of IVF.

The graph above shows the difference in the egg journey between conventional IVF and IVM both timeline wise and egg-maturity wise.
If we were to break down the fertility drugs used and timeline it injection wise, we can see quite a big difference.
Conventional IVF:
Ovarian Stimulation
FSH and LH or hMG daily injections for 8-12 days +
GnRH Agonists daily injections starting from the previous cycle post ovulation (luteal phase) or
GnRH Antagonists daily injections during stimulation phase or starting few days into the stimulation phase up until trigger injection
Triggering Ovulation
hCG single injection to trigger final egg maturation then egg retrieval done 34-36 hours post it
IVM
Mild Ovarian Stimulation (in some protocols)
FSH or hMG daily injections for 0-2 days usually but up to 3-7 days (protocol dependant)
Triggering Ovulation
hCG single injection to initiate the final stages of egg maturation then egg retrieval done 34-36 hours post it
So, for IVF we have 10-14 days of daily injections + trigger shot + daily progesterone if embryo being transferred
And for IVM we have usually 0 (but max 7 days) of daily injections + trigger shot + daily progesterone if embryo being transferred
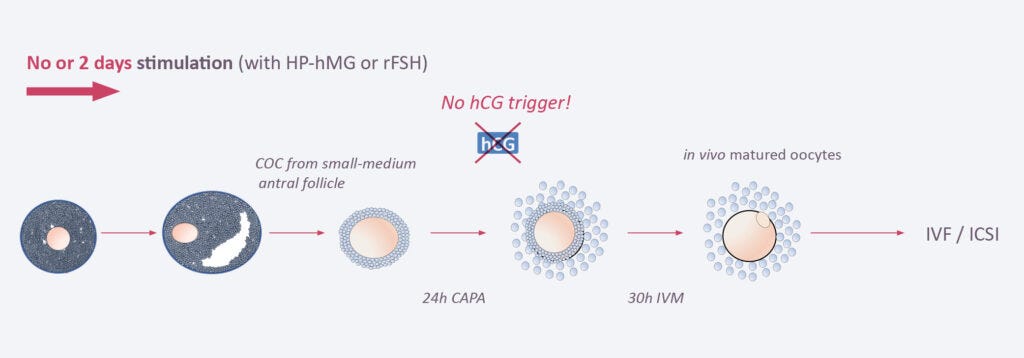
And for CAPA-IVM usually 0-2 days of daily injections + no trigger shot + daily progesterone if embryo being transferred
Those numbers are (i) dependent on protocol - especially IVM, and (ii) based on the patient and how they are reacting to them with respect to the stimulation. During the injection period, the patient will undergo blood test monitoring plus ultrasounds to ensure that the stimulation is going to plan and to minimise potential adverse effects.
2. IVM Deep Dive
I briefly mentioned above CAPA-IVM, this is a more advanced version of IVM and it stands for “Cumulus cell-oocyte complex Aspiration Prior to Antagonist treatment”. The difference is that it has an extra pre-maturation step when compared to standard IVM.
As established, IVF is associated with many injections and also the potential side effect of Ovarian Hyperstimulation Syndrome (OHS). When women get this condition their ovaries swell up and fluid leaks into the body - don’t need to be a medic to understand that doesn’t sound ideal! Some patients are more likely to get OHS, and those include women with polycystic ovarian syndrome (PCOS). Now, such women tend to undergo fertility treatments as PCOS presents with infertility.
Now, CAPA IVM is recommended as an alternative to IVF for some specific women:
those with PCOS → reduce the risk of OHS
those with cancer needing immediate treatment → many times with aggressive cancers there is no time to undergo fertility preservation treatments like egg freezing due to it needing 2+ weeks, so IVM is a suitable replacement
those with resistant ovary syndrome → women with this disease don’t have proper hormone levels and cycles (it’s also a very rare disease)
those with thrombophilia → the hormone injections increase the risk of blood clots forming, so those that are already at a higher risk of developing a clot could benefit from IVM as less hormones injected so less risk
those with egg (oocyte) maturation problems → some may experience such problems naturally in their cycle so the conventional IVF process may still lead to non-mature eggs being collected, so when you collect the immature ones via IVM you might have more chances of getting a mature one and thus an embryo
So, clearly CAPA IVM has advantages and those are:
minimal injections
minimal side effects
no risk of OHS
lower cost
Research & Literature
For the development and testing of CAPA IVM, firstly a proof-of-concept study was carried out by Sanchez et al.
The graph below shows the number of transferable blastocysts* per 100 oocytes (eggs)
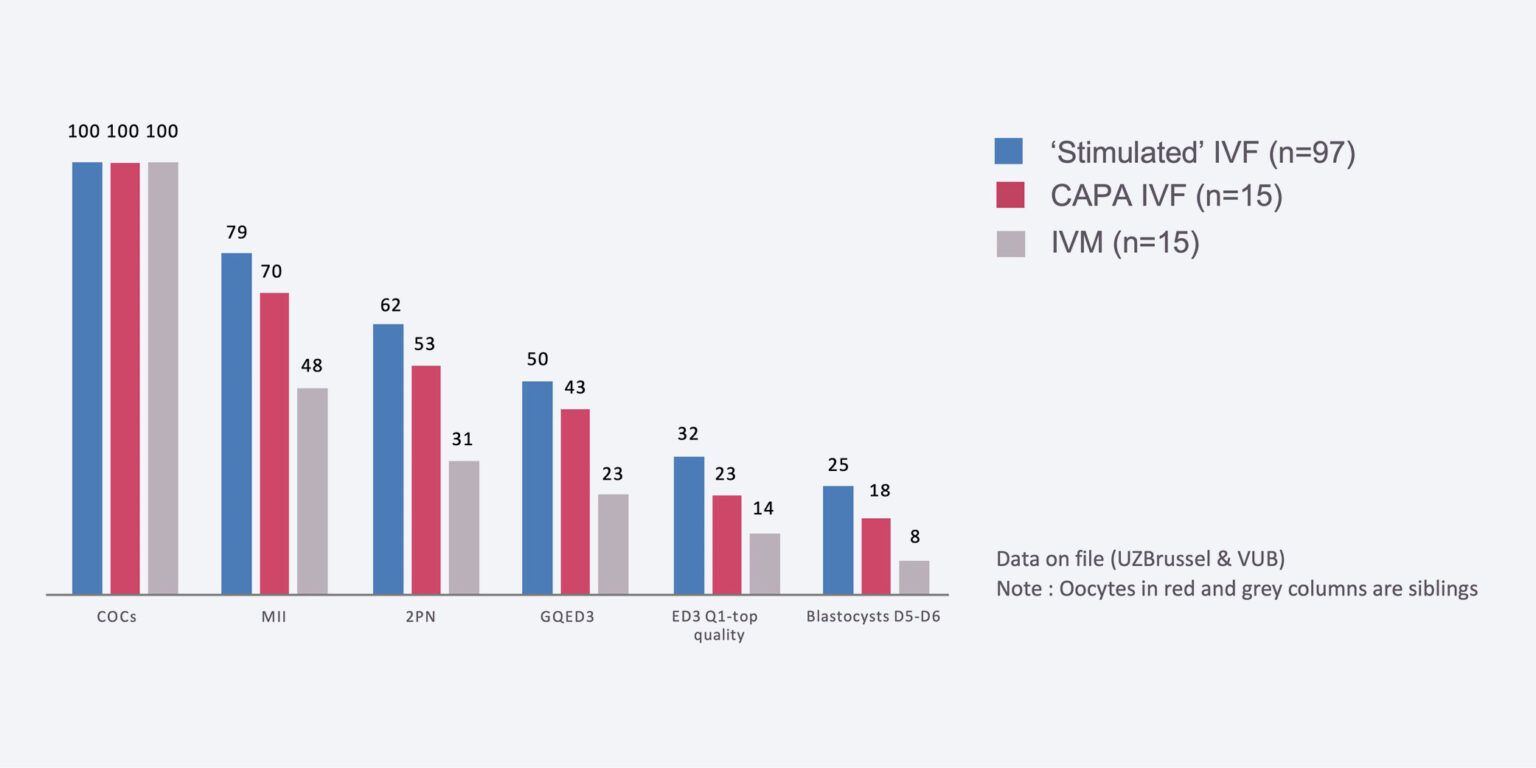
Although IVF (blue) performed the best, CAPA IVF (red) was significantly higher than standard IVM (grey).
*A blastocyst is the early stage of an embryo - it’s a cluster of dividing cells made by a fertilized egg usually happens by day 5 or 6 post fertilisation

Following the positive outcomes of the proof of concept, an RCT was carried out. The graph below shows the outcomes of it comparing CAPA-IVF vs. Standard IVF - this was led by Vuong et al.
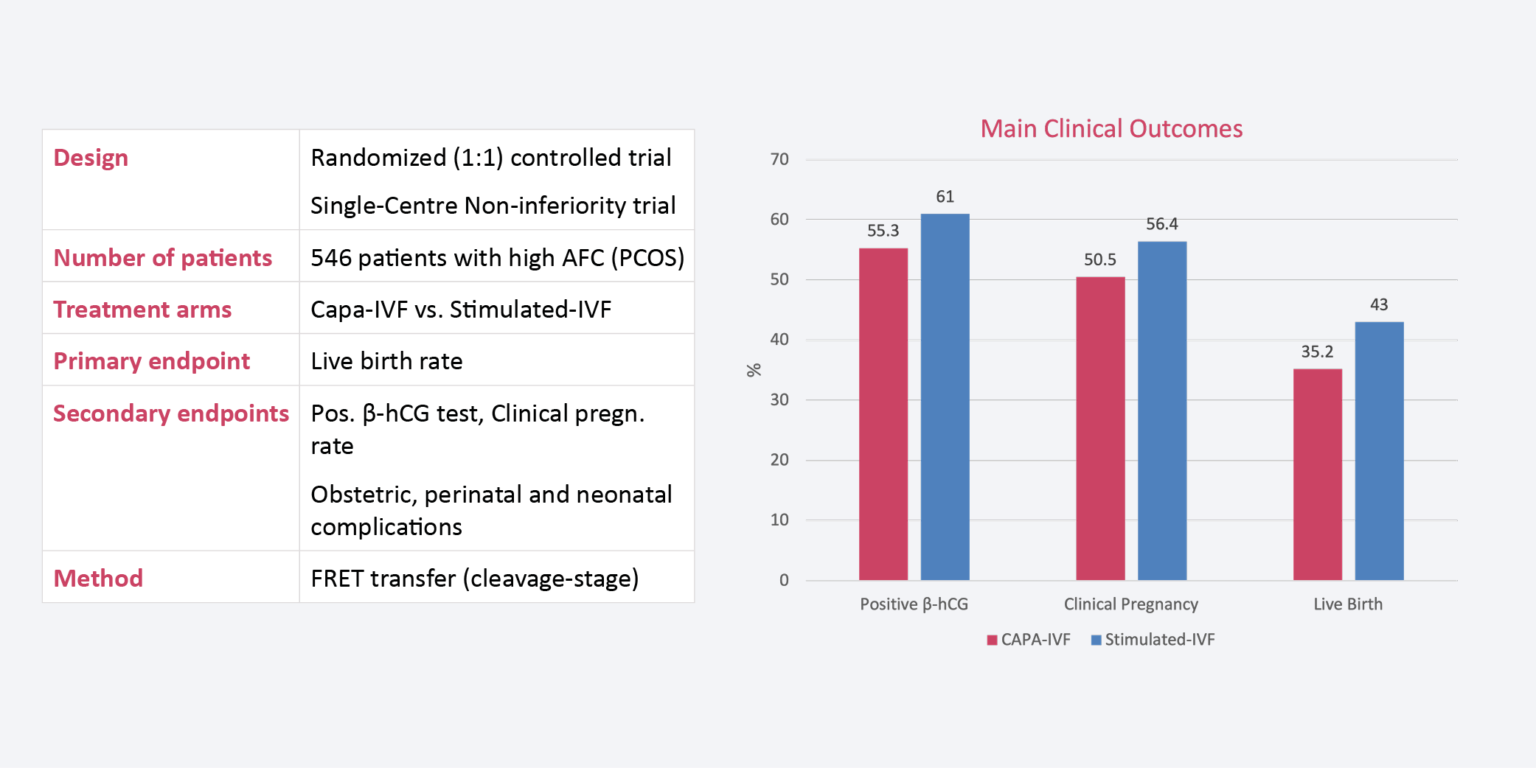
Although the clinical outcomes are slightly better in the IVF group, there were no statistically significant differences between the groups for the occurrence of pregnancy complications, obstetric and perinatal complications, preterm delivery, birth weight and neonatal complications. All the terms stated are typical clinical outcomes when it comes to a pregnancy. Also, there was no OHS cases in the CAPA IVF group but there were two cases in the standard IVF group.
Another study by Vuong et al., looked at the live births in women with PCOS and compared CAPA IVM with standard IVM. The results showed that CAPA IVM improved maturation, the clinical pregnancy rate was almost double at 63.2% vs. 38.5% (and statistically significant), the live birth rate per embryo transferred was 50% vs. 33.3% (but not statistically significant). With regards to the babies, no malformations were reported and birth weights were similar.
2-years later, Vuong et al. reported on the development outcomes of the CAPA IVM babies comparing to the IVF ones. They looked at more than 231 kids, over a 24-month period. Long-story short, they reported that it didn’t appear that there were any significant concerns on child development for the IVM babies. Which is positive news!
“The problem has been when you take an egg out of the human body it matures very quickly, even when it may not be ready to, but the CAPA method switches off the progression of the egg for 24 hours, so it grows more slowly, and it matures more healthily.”
- Professor William Ledger of University of New South Wales, Australia
3. Infertility & IVF
Considering this newsletter is called Your Medical Data Scientist, I should probably be reporting more numbers and stats. So, let’s have a look at the trends of infertility and fertility treatments worldwide and within the UK.
Infertility Trends
The WHO recently published a report on the infertility trends worldwide. I should have probably defined this earlier, but infertility is a disease of the male or female reproductive system defined by the failure to achieve a pregnancy after 12 months or more of regular attempts. There’s also primary and secondary infertility, primary is when someone has never achieved a pregnancy, and secondary when at least one prior pregnancy has been achieved. But also this is referring to a successful pregnancy.
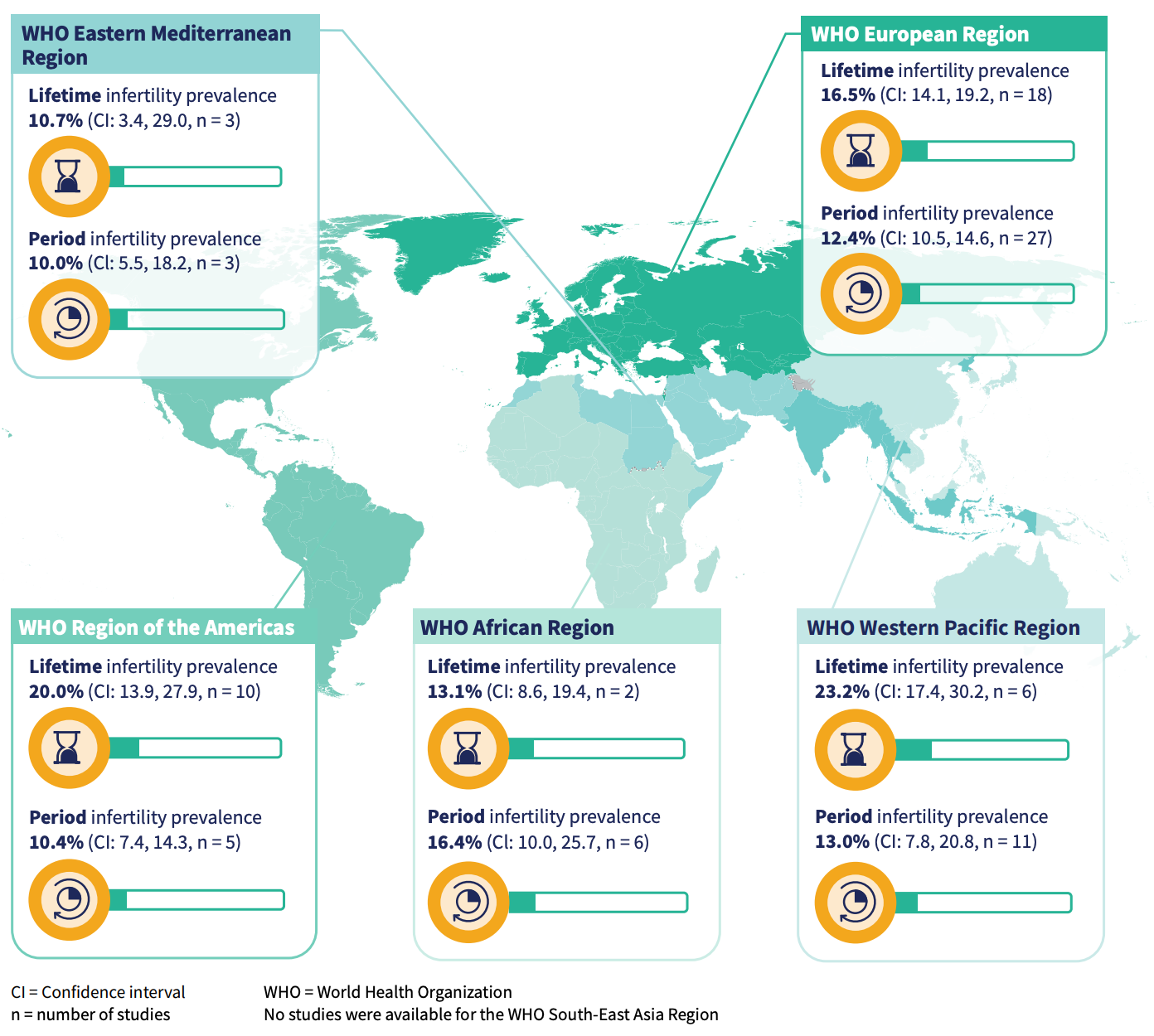
Numbers wise for 2022, 1 in 6 people are affected by infertility. The estimated prevalence of lifetime infertility is ~17.5% and of period infertility is 12.6%. Of course, this will vary by region. Lifetime is defined as the proportion of the population experiencing infertility throughout their life, and period as the proportion of the population that is experiencing infertility is a specific time interval (can be current or in the past).
The prevalence of lifetime and period infertility of the world broken down into the 5 WHO regions.
IVF Trends
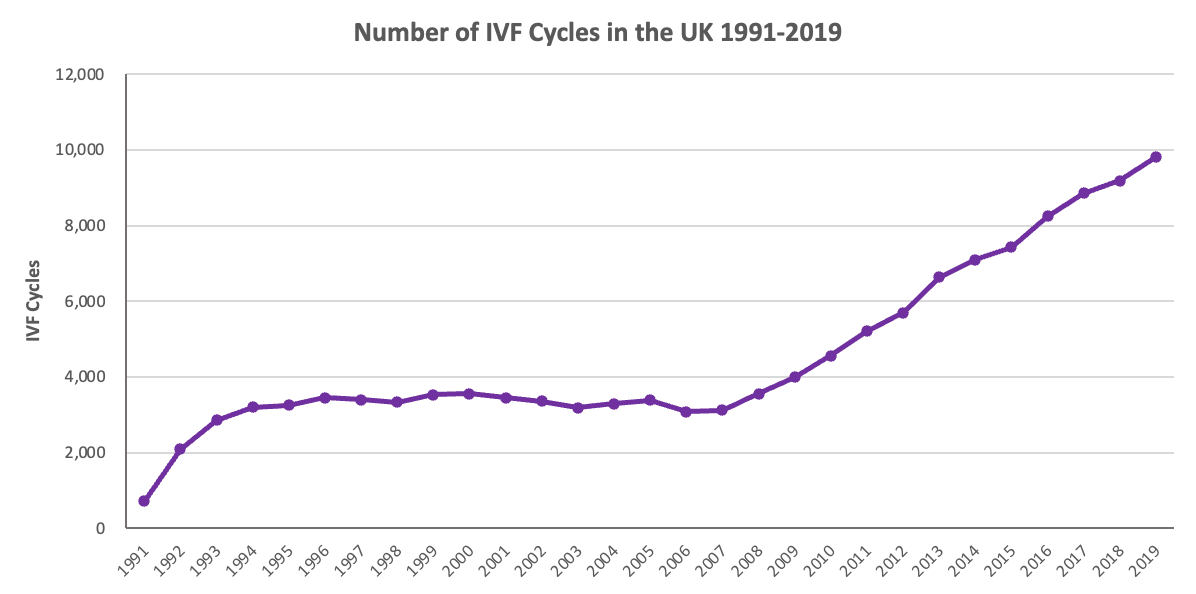
IVF is a treatment that is on the rise both within the UK and worldwide. In the UK, the Human Fertilisation and Embryology Authority (HFEA) requires that all HFEA licensed clinics provide their fertility treatment and outcomes data. This relates to the number of cycles carried out, the egg and sperm source, the cycle type, infertility causes and many more data points. Below we can see the number of IVF cycles carried out in the UK, from 2009 to 2019 the number of cycles grew by almost 250%!
In the following stacked bar chart the cycles are broken down by the patient’s age (woman) at a proportion level. As expected the 38-39 and 40+ have increased, while the under 35 has decreased. But please do note that these are proportions rather than absolute numbers, meaning that the total number of cycles of <35 may also be increasing but as a proportion to the total number it is decreasing.

IVF in the UK
Now, the NHS does over IVF treatments however under very specific conditions. They have made their recommendations using the National Institute for Health and Care Excellence (NICE) fertility guidelines as to who should access it under the NHS. Those patients are women under the age of 43 who have been trying to get pregnant through regular unprotected sex for 2 years or who have had 12 cycles of artificial insemination, with at least 6 of these cycles using a method called intrauterine insemination (IUI).
However, the final decision is made by local integrated care boards (ICBs), and their criteria may be stricter than those recommended by NICE. Which ultimately comes down to the funding received by the ICBs and Trusts, and how they want it allocated. The funding for IVF has declined over the years across England and Northern Ireland - it’s been described a bit as a postcode lottery as to who gets it. The map below shows the proportion of NHS funded cycles by the bubble sizes in different regions.

One can go privately, but (i) it’s very costly and (ii) it doesn’t come with a guaranteed successful outcome. Currently, the average price in the UK is around £13,730 to put it into perspective, that's 44% of the median annual household income (£31,400). This article explains very nicely the IVF state within the NHS.
IVF Market & Fertility Tourism
This feeds also into the financial incentives of such treatments, the fertility market itself is valued at several billion and it is projected to grow by a lot. The market has been valued at USD$1.53 billion in 2021 and said it was expected to grow at a CAGR of 7.9%, reaching USD$3.0 billion in 2030. If you think about the whole process map of the treatment there is a lot of variables that are required for one to receive treatment outside of the medical facilities and doctor fees. Equipment like microscopes, sperm analysers, incubators, cryosystems and more are needed from a lab perspective, the embryologists, the operating room and its associated costs, the drugs and hormones administered (links to pharma), the blood work and diagnostic work done throughout (hospital and healthcare practitioners).
Another big financial aspect tied to it, is Fertility Tourism - the same thing as Turkey being a destination for nose jobs and hair transplants (and a looot more). Adding a finance aspect to this, the global fertility tourism market is expected to grow at a rate of 30% over the next seven years from its 2021 valuation of USD$400 million. Barbados is a very popular destination of Americans seeking treatment, and within Europe Spain, Czech Republic, Belgium and Greece are also very population destinations.
The combination of the affordability together with the high success rates is what attracts people to go abroad for their treatment. Another aspect is the obtaining of an egg or sperm donor. In Spain, 54.3% of treatments started in foreign patients involved egg donation in 2019. Denmark is known for its sperm donors, in 2019 55.5% of donor inseminations were for foreign recipients. A big point is also the legislation around same sex couples having children, in many countries it is prohibited for them to undergo any ART treatments, thus going abroad will allow them to have a chance at starting a family.
To conclude, the birth of the first aussie IVM baby definitely marks a new milestone in the evolution of ARTs. Considering the lower cost and that it’s less invasive this could make treatments much more financially accessible and patient-friendly. It’s definitely exciting times in the fertility-related healthcare industry for patients worldwide! It’s great to see how the technology is involving and new innovations are being created that are safe to use and successful! Now, that being said long term studies need to be carried out with regards to the development of IVM babies and the potential adverse effects arising, like those done for the IVF babies (which have no more developmental than normally conceived babies).
Ultimately, unless the cause of infertility is disease related, both men and women should pay attention to their health as it has a direct impact on their fertility. Outside of systematic causes (e.g., endometriosis or prior chemotherapy) there are many factors that affect one’s fertility which can be mitigated and improved on. A major one is stress, that has been proven to interfere with a woman’s ability to get pregnant (think cortisol spikes and the overall endocrine / hormonal system). The fact that we are also an increasingly growing population, weight-wise that is, is also directly related with decreased fertility. Another point is the patient’s age, as we age our fertility drops but this is much more apparent in women than men, however, considering the fact that people opt to have children at a later age it implies that by the rule of numbers more will end up needing fertility treatments.
So, I shall leave you with a quote form the father of IVF, Robert Edwards which was also the 2010 Nobel Prize Winner in Medicine.
“The most important thing in life is having a child. Nothing is more special than a child.”
- Robert Edwards
As usual, I've provided some references below. See you next week! :)
Further reading / resources:
Abbreviations:
ART - assisted reproductive technique
CAPA-IVM - capacitation in-vitro maturation
FSH - follicle stimulating hormone
hCG - human chorionic gonadotropin
HFEA - human fertilisation and embryology authority
hMG - human menopausal gonadotropin
IVF - in vitro fertilisation
IVM - in vitro maturation
LH - luteinising hormone
OHS - ovarian hyperstimulation syndrome
PCOS - polycystic ovarian syndrome