

Endometriosis: A Silent Disease
Endometriosis: A Silent Disease
An invisible yet painful disease.

Endometriosis (endo) is classified as one of the most painful conditions, it only affects women, more specifically 1 in 10 women of reproductive age have it. When a woman has endometriosis, the lining of the uterus grows in other locations outside of the inner uterine wall, typically it is found around the other organs of the reproductive system (ovaries, fallopian tubes, etc.) and generally in the pelvic cavity. However, in some rare cases it can be even found outside of the abdominal area, for example on / around the lungs.

Unfortunately, the cause of it is still unknown but a family history of it has been established as a definite risk factor, alongside heavy long periods, and infertility. That being said with the latter, it is not the case that infertility is the cause of it, however, this is usually the way one gets an endo diagnosis since they are having trouble conceiving. When looking at it from a patient pathway perspective, this also makes sense as it takes on average between 6 to 10 years to get a diagnosis, which technically is only “official” if confirmed via laparoscopic (key-hole) surgery. Endometriosis is very much one of those conditions where it is a diagnosis of exclusion, like IBS.
The main symptom is pelvic pain, mostly during menstruation but not only then. Periods are usually heavy, some may be irregular, and there may also be bleeding in between cycles. Other physical symptoms like abdominal pain, fatigue, and gut issues may also present during periods which are common for a multitude of conditions. The symptoms are not always present with everyone, and they vary a lot making it a heterogenous disease. The variety of symptoms is not what makes it heterogeneous, it is at a macroscopic level where lesions can look similar in reality they are not, and that is the reason why different symptoms and behaviours are exhibited.
As stated earlier, to be officially diagnosed with endometriosis one needs to undergo laparoscopic surgery, a further reason for that is that after the operation the samples excised are sent to histopathology like a tumour is sent for a biopsy. Not all surgeries result with a sample being sent for histopathology, as once the doctor can see the organs they can differentiate between endo and say ovarian cysts or some tumours being present. Prior to surgery other diagnostic attempts would include pelvic examinations, ultrasounds, and even MRI scans.
If the surgery confirms that there truly is endometriosis a sample is usually removed and biopsied. Based on those results this can guide the doctor and patient deciding on which is the most appropriate manner of treating the condition. There are three main types of treatments offered:
Medication used to alleviate the pain
Hormone therapy
Surgical interventions for the removal of the endometriosis
There is currently no cure for endometriosis, like most of women’s conditions, so the treatments are classified as medical and symptomatic and implemented to improve quality of life.
Medication: This typically is non steroid anti-inflammatory drugs (NSAIDs), which are drugs like aspirin and ibuprofen. Currently there are no endometriosis specific pain drugs.
Hormonal treatments: There are a few hormonal treatments that are being used. All of them have the goal of reducing the amount of oestrogen circulating in the blood and body. The two general options are the combined oral contraceptive pill and the progesterone only pill. The combine pill is to be taken daily, but for the progesterone may be taken daily as a pill, or an arm implant, or via a coil (like Mirena).
There are two other types of treatments that are classified as hormonal, those are gonadotropin-releasing hormone (GnRH) Analogues and Aromatase Inhibitors (AIs). GnRHas are a synthetic form of the hormone gonadorelin which suppress the production of luteinising hormone (LH) follicle stimulating hormone (FSH) - which are reproductive hormones by directly acting within the pituitary gland. Like the contraceptive pills, AIs suppress the synthesis of oestrogen in the ovaries and peripheral tissues. Aromatase is an enzyme that converts androgens to oestrogens, so the inhibitors block the action of the aromatase which means there’s less oestrogen circulating the blood.
Surgery: Like the surgical laparoscopic diagnosis, such procedures may be undertaken again for the removal of the endometrium. However, around 1 in 5 women do not see any improvement in their symptoms post surgery which comes with the usual risks of any surgery. Potential long term effects also include the creation of abdominal lesions, which basically is scaring tissue of the organs. This scarring tissue is directly linked with chronic abdominal pain just like endo.
Fertility & Endometriosis
As mentioned earlier, a lot of women get an endometriosis diagnosis when in the process of getting pregnant and discovering they are having fertility issues. Aside from women having difficulty getting pregnant, having endometriosis puts one at a greater risk of miscarriage; that is one of the reasons that a lot of women undergo in vitro fertilisation (IVF) treatments, although as a disease it has a negative influence on the IVF outcome, there are still high chances of success.
In 2010, Pasta and Adamson proposed the endometriosis fertility index (EFI) - a scoring system used to predict the pregnancy rates in women with surgically diagnosed endometriosis not undergoing IVF conception. Previously, the revised American Fertility Society (rAFS) score was used which was developed in 1997 by the American Society for Reproductive Medicine, however, it was not deemed effective enough in predicting the clinical outcomes of pregnancy rate in infertile women, and hence why EFI was designed. A copy of the EFI scoring card is illustrated below.
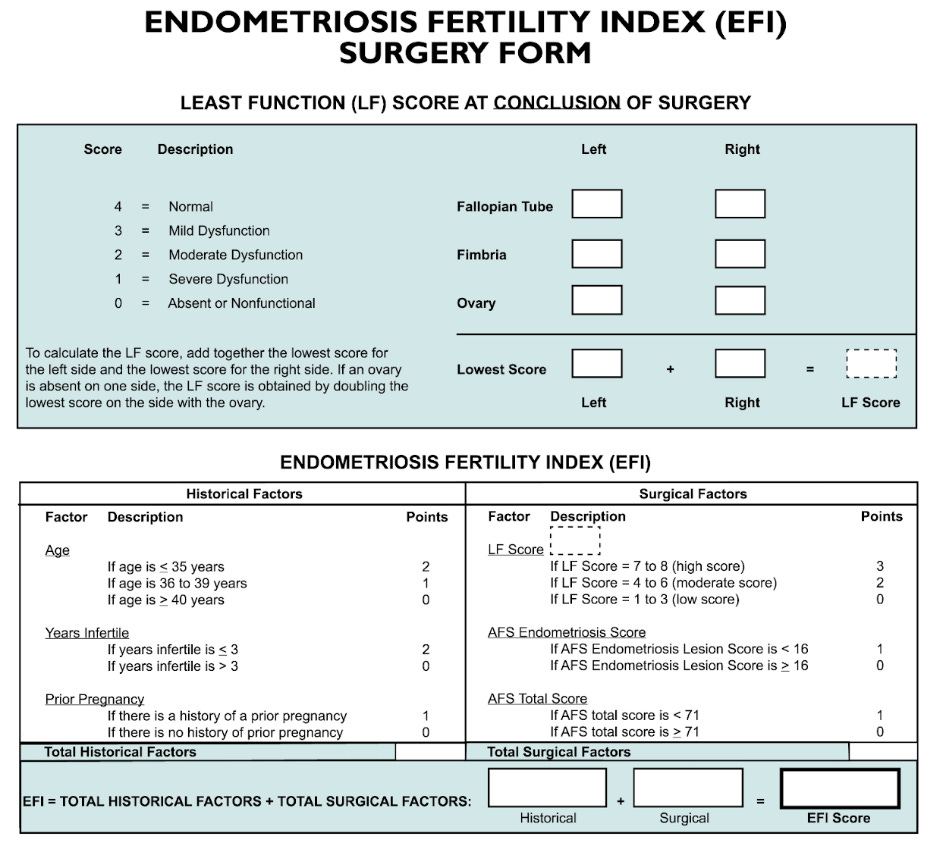
The patient gets a score out of 10 allocated, with 0 being the poorest prognosis and 10 the best. The points are evenly split between historical and surgical factors. Based on the EFI score allocated, there is an equivalent estimated pregnancy percentage.
UK Statistics & Education
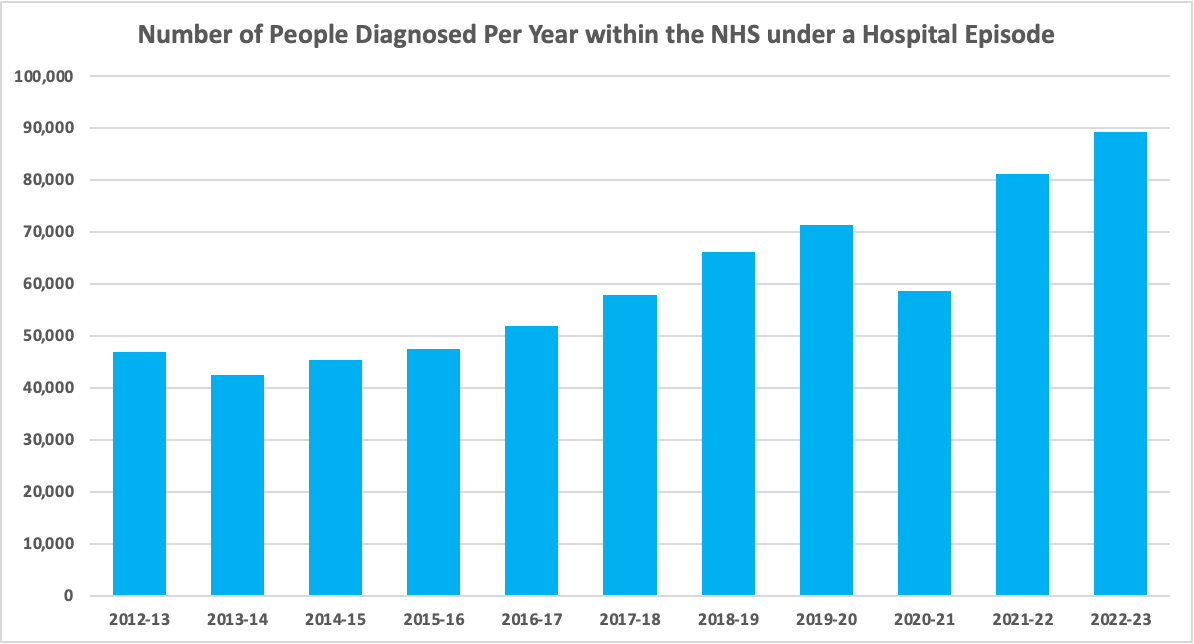
The NHS publishes yearly data regarding the hospital admitted patient care activity, of which one of the datasets is on diagnosis codes. The graph below shows all patients having a diagnosis of endometriosis (both primary and non-primary) as part of their hospital spell. As shown, the number of women being diagnosed is continually increasing, aside from 2020-21 which was impacted by the COVID-19 pandemic. The number of women diagnosed with endometriosis has grown two-fold from around 45k in the early 2010s to 89k in 2022-23.
Although endometriosis is still very much an unknown cause, a lot of work is being done to raise awareness like the introduction of the endometriosis awareness month which occurs every March. This may also be the reason that more and more diagnoses are being made as doctors are more familiar with it. In the UK, more than 50% of the women went to A&E for abdominal pain due to endometriosis, prior to having a diagnosis of what this is as per the all party parliamentary group on endometriosis.
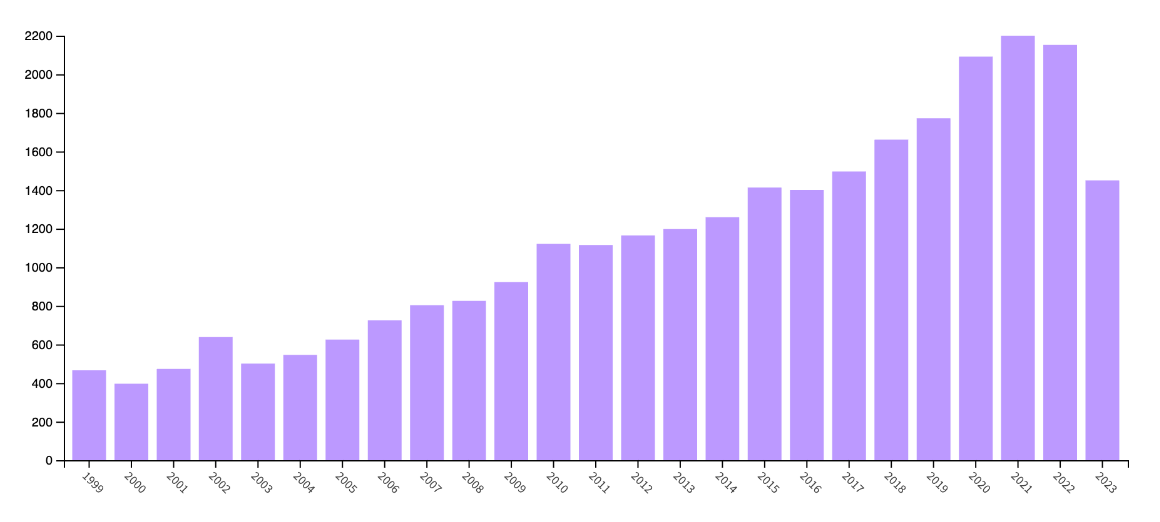
General education, both within the public and the healthcare professional is not where it should be. This may also be seen as the National Institute of Health and Care Excellence (NICE) first published its guideline for the diagnosis and management of it in 2017, and it has not been updated since. There has been an increasing amount of research being carried out, as seen in the graph below which shows the number of publications relating to Endometriosis (accessed via Web of Science).
To summarise, the lack of a reliable diagnostic test for endometriosis alongside the fact that a specific endometriosis targeted treatment does not exist is frustrating for doctors and patients alike. More research is constantly being done, with leading research groups like that of Oxford University - Endometriosis CaRe and the Adelaide Endometriosis Research Group in Australia. There are online support groups emerging, on social media platforms like Reddit, Facebook, and Instagram which aim at both raising awareness but also supporting women.
Hopefully in the near future, with the advancements in personal medicine, and the studying of endometriosis both in terms of aetiology and pathogenesis, more solutions may be available for such a prominent condition with a negative direct impact on quality of life. With the collation of data over time, the condition should be better understood and treated at an earlier stage which would also reduce its severity if diagnosed at an earlier stand point.